The Era of Opioids As the Gold Standard for Pain Management Is Over

The Majority of Surgical Patients Receive Opioids & Many Will Go On to Become Persistent Long-Term Users1,2
While opioids have been a mainstay in postsurgical pain control, they are also at the center of an ongoing national crisis. For many patients undergoing surgery, it is their first exposure to opioids.
99% of Patients
receive opioids to manage postsurgical pain2*

1 out of 15 Surgical Patients
prescribed an opioid may go on to long‑term use or abuse3,4†
An Estimated 1.1 Million Americans
will become persistent users of opioids each year following initial exposure after surgery in the hospital3
*In a retrospective study of hospital discharge data (N=37,301)
†In a prospective longitudinal study (N=109)
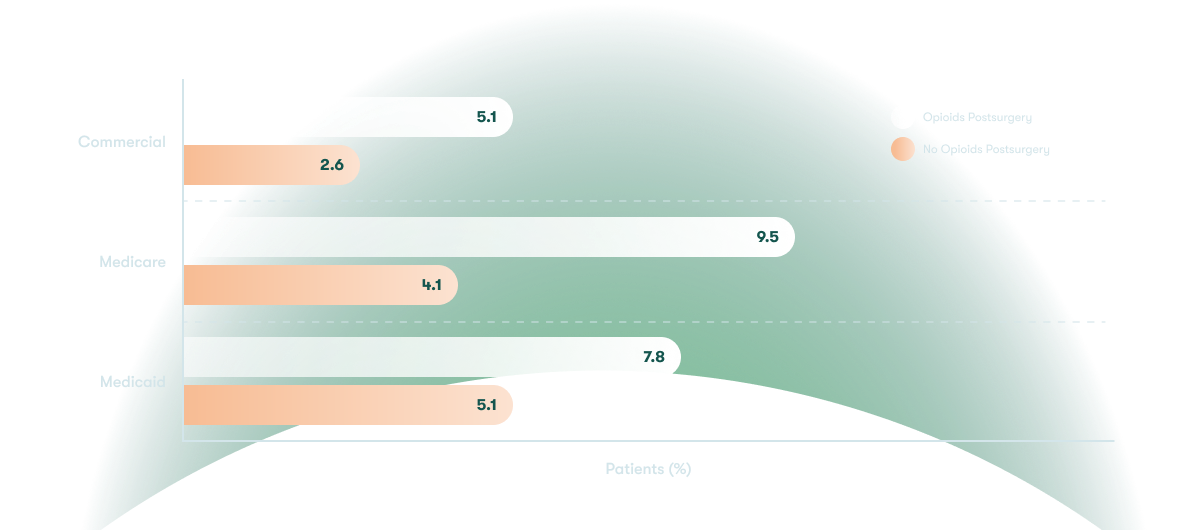
Newly Persistent Opioid Patients by Percentage

Economic & Clinical Burdens of Opioid Use in Multiple Payer Channels in the United States1
Study Background
Retrospective, observational cohort study of medical claims, healthcare utilization, and costs in opioid-naive patients who received and those who did not receive opioids after surgery in large, nationally representative claims databases
Patient Population
- N=4,105,121
- General, orthopedic, plastic, obstetric/gynecologic, and other surgery
Findings
Postsurgical opioid use resulted in increased total inpatient healthcare costs, increased inpatient and outpatient postsurgical pain, and increased outpatient admissions/readmissions
Total Healthcare Costs (Inpatient)

Swipe left on chart to see more
Postsurgical Pain Within 90 Days
| Commercial Patients | Medicare Patients | Medicaid Patients | |
|---|---|---|---|
| Opioids Postsurgery (Inpatient) | 1.9% | 2.5% | 2.8% |
| No Opioids Postsurgery (Inpatient) | 0.7% | 1.2% | 0.7% |
| Opioids Postsurgery (Outpatient) | 7.6% | 4.5% | 6.5% |
| No Opioids Postsurgery (Outpatient) | 1.8% | 0.6% | 1.8% |

Swipe left on table to see more
Admission/Readmission Within 90 Days (Outpatient)
Swipe left on chart to see more
There Are Risks Associated With Opioid Exposure
68% of People
using pain relievers (non-medically) obtained them from a friend or relative7*
4 out of 5 New Heroin Users
started out by misusing opioids8†
*According to the 2013 National Survey on Drug Use and Health among past-year users aged ≥12 years (N≈37,000)
†From an analysis of the 2008-2010 National Surveys on Drug Use and Health to examine patterns of heroin use and risk behaviors among past-year non-medical users of opioid pain relievers
Most Patients Would Prefer a Non-Opioid Option to Control Their Pain After Surgery9*
~90% of Patients
said they were concerned about side effects of, addiction to, or dependence on opioids
79% of Patients
said they preferred a non-opioid pain management option
*From a survey of 500 adults in the United States who had an orthopedic or soft tissue surgery and 200 US surgeons who perform these procedures
